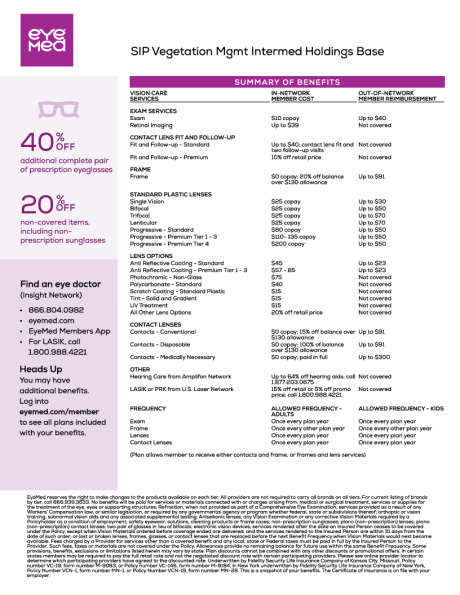
Vision Plan This year we are proud to offer two vision plan options for employees through EyeMed. The chart below is a brief summary of the in-network benefits. Please refer to the specific plan documents below for complete plan details. Plan Highlights Base Plan Buy-Up Plan Member Responsibility In-Network In-Network Routine Exams $10 $10 Vision Materials Frames 20% off balance over $130 20% off balance over $200 Contacts - Covered in lieu of frames Conventional Contacts 15% off balance over $130 15% off balance over $200 Disposable Contacts 100% of balance over $130 100% of balance over $200 Medically Necessary Contacts No charge No charge Standard Plastic Lenses Single $25 $10 Bifocal $25 $10 Trifocal / Lenticular $25 $10 Progressive $80 - $200 $65 - $185 Frequency Lenses - in lieu of contacts Once every plan year Once every plan year Contacts - in lieu of lenses Once every plan year Once every plan year Frames Once every plan year Once every plan year Exams Once every plan year Once every plan year WEEKLY RATES WEEKLY RATES Employee $1.66 $3.46 Employee + Spouse $3.15 $6.57 Employee + Child(ren) $3.32 $6.92 Employee + Family $4.88 $10.17 Please refer to the summary plan description for complete plan details. EyeMed website Plan Documents Vision Base Vision Buy Up Vision Insurance prevDental Telemedicinenext